Have you ever calculated how much urine and sweat are in the average pool? The number might surprise you. All this urine and sweat (amongst other things) form that nasty, elusive thing we know as chloramines, which show up as the combined chlorine we see in our daily tests.
This tells us what’s in the water, but not always what’s in the air. Nitrogen trichloride, aka trichloramine (TCA), literally jumps out of the water and into the air. But what is it made of? Three chlorine atoms attached to the ammonia ion, which comes from urea, the main component of urine and sweat. So if you have a lot of chlorine in the water as well as a lot of urine and sweat, then you’re going to have combined chlorine, the precursor to TCA. We can make an assumption that if there’s a lot in the water, then it is likely there is a lot going off into the air. That’s what we know today.
We knew even less in February 2007. A new Great Wolf Lodge in Mason, Ohio, had an issue no one could put their finger on. It wasn’t until we had done a lot of research and testing that we thought we found some solutions.
None of us knew at the time that these valuable lessons learned would impact the development of the ventilation module of the Model Aquatic Health Code.
We knew developing the ventilation module would be a challenge because the spectrum of indoor aquatics facilities is wide and water treatment also is needed to include new technologies that are not in widespread use.
What worked for one facility might be overkill for the other, so we had to think of how to approach this without adversely affecting either end of the spectrum. It was apparent we would need a diverse group to be on the technical committee, so we selected a team of experts with specific backgrounds: academics, sanitarians, government specialists in industrial hygiene, facility operators of varying types of facilities, designers, manufacturers and ASHRAE experts.
We had some very lively discussions on the various aspects of indoor air quality, then we broke these down into sections so we could systematically address them.
- Which contaminants are in the air based on peer-reviewed science
- The effects these contaminants have on people, and which contaminant thresholds were already established in current research
- How these contaminants get into the air so we could address the mechanism of entry
- What the hierarchy of design should be (bather comfort vs. building protection)
- Parameters for smaller, low bather facilities with low ceilings vs. high occupancy facilities with huge air volumes
- Requirements for pools with basic water treatment vs. those with sophisticated systems designed for managing contaminants
- How facilities are maintained by on-site staff
- How to address the contaminants brought in by bathers
- How to write a code that would be practical, meet the objective of improved air quality and yet could be enforced by sanitarians
We discussed all the objectives outlined above, but we also had three distinct conversations about contaminants and thresholds; fresh air requirements; and the use of UV and ozone to minimize airborne contaminants.
Very early on in the discussions, we evaluated the known biological and chemical contaminants present in the air and determined their prevalence and adverse effect on bathers. The research pointed to TCA being most prevalent and the compound having the most well-known adverse effect. But we also had a challenge in determining what would be an acceptable threshold in an indoor environment.
First, the test method used for TCA in the research varied, so that meant the amounts recorded could be different among the research. Second, there is no easy test that a sanitarian or operator could use in the field that would allow for a real-time test as we have for testing free chlorine, pH and the like. It would be difficult to enforce a threshold that could not be easily measured. As a result, the ventilation module has not proposed thresholds, but as technology develops for real-time testing, we may be able to incorporate measurable and enforceable thresholds into future editions of the MAHC.
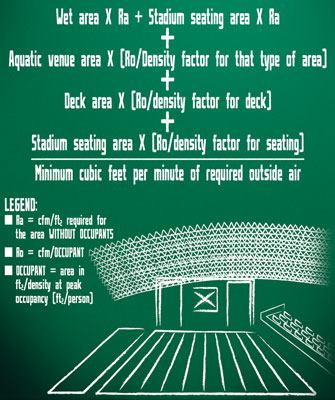
As we considered airborne contaminants, we discussed the fact that under current practices, the most common solution was bringing in fresh air. This removed contaminants and diluted the amount of contaminants regardless of the type. We had a “think tank” session in which a formula for fresh air was established.
Using ASHRAE requirements as a base, the group developed an amount of fresh air required to not only account for the building size, but for the types of pools, and the number of people in these environments. This helped us address small and large facilities, as well as low bather vs. high bather load facilities.
The approach was practical, considering the density of people in pools and the fact that certain pools contribute to air quality differently. Moving water releases TCA more than flat-water pools. Hot water releases more contaminants in the water, and evaporation releases more TCA into the air. The formula used for determining the minimum fresh air requirements is modular, so it will not limit design.
Lastly, we discussed the use of UV and ozone as a method to control combined chlorine in pools and hence remove the precursors to TCA. The problem is, the types of equipment on the market vary greatly and how they are installed determines their efficacy. To know definitively that UV or ozone would be effective, a test method would be needed to prove the equipment’s efficacy under certain conditions. Without the research to show the efficacy, we had to rely on what we know works and could be measured.
As a result, the backbone of the ventilation module is the formula for determining fresh air requirements. We think this will help designers plan for fresh air, not just based on the square footage, but also peak occupancy and type of pools (for example, flat, agitated and hot water). We believe it is practical and reflects the standard practices in how water quality is maintained. It also adds safety factors for air handling based on contamination burden. We hope you find the same as you read through the document posted for public comment through June 12 on CDC’s Healthy Swimming Website. Your input and comments are appreciated and will be considered even after the June 12 date!

